Multiple Gated Acquisition Scan
MUGA Scan
_____

Well it may look scary! but it’s not, oh and it doesn’t hurt either.
This is my second scan, I had one during my transplant assessment
Well, why and what? Muga scan in my words, it is to check the function of the left side of the heart. First you have a injection approx 20minutes before the scan, the reason for this is so that when you are given the second injection that has the radio active ingredients in it (real medical terms?), the radio active part only attaches itself to your blood cells and not other organs or areas of the body, that don’t need to be tested. So you have the first injection, then 20minutes later you lay down on a bed where the scanner is, then you are given the second injection. At this point you are also connected to a E.C.G. machine, the scanner is moved into position and now you just relax for about 10minutes (they played a jazz C.D. for me at this point). Then much to my surprise it was all over, off with the E.C.G. stickers, up and out.
Because it is you that is radio active you need to avoid pregnant women and young children for the next few hours (prolonged contact that is). Oh and no you don’t glow in the dark, not that I tried it or turn into the hulk.

Just relaxing and listening to jazz C.D – E.C.G. sticker being applied.

This is Emma Wilson who did the scan for me and took the pictures.
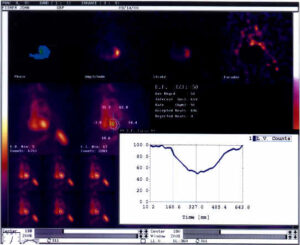
The results of my scan, sorry there hard to see/read but even harder for me to explain, Either I will have to read up on it or better still convince Emma that she wants to write about it for me (watch this space)
“NUCLEAR MEDICINE”
Aaaargh…..what is it, it sounds awful!
Does it hurt? I don’t like the idea of being radioactive!
Will I glow in the dark?
What about being with other people?
In nuclear medicine clinical information is derived from observing the distribution of a pharmaceutical administered to a patient. By adding a radionuclide into the pharmaceutical, measurements can be made of the distribution of this radiopharmaceutical by acquiring an image on screen.
The science: Ionizing radiation is any form of radiation that has sufficient energy to release one or more electrons from around the atomic nucleus to which they are normally bound. The common forms of radiation in medical use are X-Rays, gamma rays and beta particles. The main difference between the ionizing radiation produced from radioactive materials and that of X-Rays is that nuclear emissions originate within the nucleus of the atom, whereas X-Rays are produced from the electron cloud surrounding the atom.
With Nuclear Medicine scans, a small amount (usually about 0.1 – 1.0 ml) of radioactive fluid is injected in the arm (just like giving a blood sample) and a scan is performed, depending what is being looked at, at a set time later. You are then classed as being slightly radioactive. This means that you have had the injection and should avoid close, prolonged contact with any pregnant ladies or young children for 20 – 24 hours after the injection. This means avoiding going straight home to cuddle a baby for 12 hours or sleeping with a pregnant partner. This is to avoid giving those more sensitive / growing people any increase in the natural background radiation they are receiving anyway. There is natural background radiation around us all the time, coming from the atmosphere, the earth and equipment. The aim is to keep it all in perspective and only use it medically under strict guidelines and if necessary for your benefit. There is no need for concern if you listen and understand what the radiographer tells you on the day. If you apply the rules of the inverse square law (remember physics!) that is enough to know. Bear in mind that the radiographers doing your scan could well be young females and are with ‘radioactive’ patients all day, in close contact, and are still working there…. If there was anything to be worried about we wouldn’t still be here!!!
NO it doesn’t hurt and NO there are no side effects
MUGA SCAN:
This is a routine test done to assess and monitor the function of your heart pre and post transplant. Its main role is to calculate the EJECTION FRACTION of the LEFT VENTRICLE (the main pumping chamber of the heart), that is to calculate how much oxygenated blood is being pumped out to the body.
Echo cardiography (ultrasound) is done more frequently to monitor left ventricular performance, as it can be performed at shorter intervals, as it does not involve any irradiation.
MUGA stands for MULTI GATED ACQUISITION – this means that we are acquiring a scan using a gated ECG signal from your heart. ‘Gated’ means that the ECG wave is split into 16 or 32 frames per R-R interval (one heart beat / signal).
R R
(Excuse the freehand drawing)
At the end of the scan there may be over 1000 heartbeats worth of information accumulated into one simulated heartbeat / cycle. This sequence is then viewed to assess heart wall motion. Regions of interest are then drawn around the heart when it is full (diastole) and when it has contracted (systole). The difference between the two stages provides you with the ejection fraction – usually 45% and above.
Patients that are being assessed for a heart transplant, usually have a low ejection fraction.
John had a MUGA in September 1999 and had an ejection fraction of 8 % !!! (according to our scan, echo may well have given a different figure as it calculates the ejection fraction in a different manner). His curve would have looked very similar to the first one below.
When John visited us last week, September 2000, one year later, his ejection fraction was 50%.
The scan involves having 2 injections – the first is of something called stannous pyrophosphate – this binds to red blood cells and makes the second injection of the radioactive tracer ‘bind’ / label to the red blood cells and hence allow imaging of blood flow.
The patient is now the “X-Ray”, emitting gamma rays that are detected by the gamma camera, which is crudely acting as a big Geiger counter, which accumulates information coming from the patient into an image on the computer screen.
You will lye down on a couch for about 10 minutes, with 3 leads from the ECG on your chest with the camera to your left hand side. IT IS NOT an enclosed machine (see photos of John).
Above are the curves you would expect to see for left ventricular function pre and post transplant. The first ‘flatter’ curve indicates a poorly functioning left ventricle – little activity/isotope is moving from the heart into the body.
The second curve indicates a left ventricle that is working well – there is a definite emptying and filling phase showing.
The above is just one persons overview of Nuclear Medicine and MUGA scanning, in order to give you, the patient, a better understanding of our department. Other professionals may read this and want to add comments – please feel free.
Emma Wilson
Transplants Save Lives
We totally rely on donations to fund the charity, including this website which has remained free for over 21years.
We are very reluctant to add google ads etc, so please make a small donation to help pay for the day to day running costs of the charity and website.
Note we are non-profit and run totally by volunteers.

To Transplant & Beyond is a UK registered non-profit charity No 1106248
© 2000 All rights reserved